Charles E W Bean, Diaries, AWM38 3DRL 606/251/1 - 1915 - 1936 - Part 16
Jan, 1915-June, 1916) THE SERVICE IN AUSTRALIA 525
deformities and diseases of which the military significance
is notoriously difficult of exact appraisement, even if they can
be detected. During the first year of the war approximately
thirty-three per cent of all volunteers were rejected. In
June, 1915, the standard of height was lowered to 5 feet
2 inches. With the establishment of a dental service the
fitness of recruits, from the standpoint of that profession,
became a matter merely of the time necessary for their
treatment, for which an effective procedure was built up
by this new and zealous department. Provision was made
for the enlistment of men who required both upper and
lower dentures, and this naturally rendered available a large
body of men otherwise ineligible. As a result of reports
from the ophthalmic specialists, the eyesight tests were
slightly relaxed and the use of spectacles was permitted.
Venereal disease was put on the same basis as dental
unfitness.
In respect of the medical examination itself; the
irregularity of recruiting made exact arrangement difficult,
and it is evident that no very precise procedure was built
up. In general the policy was adopted of making the
examining medical officer personally responsible, and of
seeking his co-operation in overcoming the difficulties connected
with the detection and rejection of unfit men among
the recruits. Toward the end of 1915, however, “standing
medical boards” were appointed to pass or reject all recruits
“about whose fitness there was doubt,” and, in order to
suppress impersonation, repeated re-examination before
embarkation was ordered.
The unexpected developments in regard to enteric diseases
in the latter half of 1915 brought about something of a crisis
in the matter of anti-typhoid inoculation as a condition to
enrolment. Early in the year reports from Egypt of the
absence of typhoid had been hailed as evidence of the
Value of efficacy of the procedure. No greater
inoculation danger besets the medical profession than
questioned that of premature wresting of evidence to suit
current theory, and this hasty and unfounded
optimism was soon shaken. By June the occurrence of cases
diagnosed as “typhoid” in the troops at Gallipoli was
misdated 29/3/18
28/3/18
1.25 p.m.
C.O. 38Bn.
Position now as folls.
DLI have one coy dug in the line running N & S through R
in Treux to edge of wood, thence S along sunken road to first
B an ABBE, thence along S.E. edge of wood. When all their coy
cdrs reports they hold a continuation of this line N but I have not
yet confirmed.
Enemy in considble strength [unable to estimate nos] Can be observed
digging in along a line 'ridge 60 south to P in Post. He is also
moving by parties of ones and twos from Morlancourt to
timber S.W. of V in Ville.
His m/gs snipers are very active on E edge of wood
especially along sunken road running south from Treux. Several
470 THE GALLIPOLI CAMPAIGN (1915
From the technical side the surgical work does not call
for description in detail. It is not, however, without interest
"Immediate" to note comparison with procedure elsewhere
surgery the principles laid down for the
Gallipoli campaign by the consulting surgeon,
M.E.F., in connection with the "immediate" surgery
recommended in certain special types of wound.
Abdominal wounds.— A morphia injection to be given and all food
and fluid by the mouth forbidden. They bear transport badly, and
should be moved as little as possible for the first few days. If they
reach a hospital or hospital ship within a few hours of injury and
are seen by an experienced surgeon, he may consider it wise to
operate in exceptional cases but as a rule expectant treatment gives
the best results.
Head injuries.—Bear transport badly and should be operated on
early, depressed bone being removed, the wound ascepticised and
drained but not stitched.
Chest injuries . . . from gunshot wounds, unless rapidly fatal,
as a rule do well and should not be interfered with. Haemorrhage, if
dangerous, tapped by a trochar; incision and drainage if it repeatedly
collects.
Amputations should be rarely resorted to unless the limb is
smashed up.
Those surgeons with No. 3 Australian General Hospital
who had seen service in France found that their experience
at that seat of war was in some degree misleading, in that
at the Dardanelles not all wounds demanded, as in France,
opening up and drainage.
Speaking generally, it is probable that after the end of
August the conditions on the lines of communication from
Gallipoli were, for all cases, as good as on the French front
[*/s *] at this time; for the ^slightly wounded throughout the
campaign they were better.
At the base, the vast majority of seriously wounded Australians
went to the British hospitals at Alexandria. Almost
At Base all the major "secondary surgery" and much
"primary surgery" in connection with the"
Australian wounded was carried out in these units. No
records are available of their work: but evidence makes
it clear that, from June onwards, a high standard was
38 Even Gallipoli experience was in some instances at variance with this advice.
An Australian surgeon working on hospital ships assessed his successful immediate
sections at 33 per cent.
2.
small patrols often seen working forward from enemy line
At 1.10 pm a party of enemy estimated at abt 25
with 2 MG's attempted to advance but were driven back
by our arty, L G and rifle fire. Our L G's caused him
several casualties.
Position now quiet.
A Coy of Lancs Fus has just arrived to take up a
position on the edge of the wood. Am going to
look at their dispositions.
F E Fairweather
O.C, "C" Coy
Treux Wood
(29). 3.18
this should surely be 28th
1.25 p.m. by Capt Orchard.
Received 1.55 p.m.
1915] SURGERY 469
operating was restricted both by lack of opportunity and later
by definite order. At the end of July the Principal Director
of Medical Services was instructed by the War Office -
to call the attention of surgeons aboard hospital ships to the necessity...
for limiting operations to those which are absolutely necessary
Flap amputations should not be performed. Sutures should not be
employed either in amputations or in deep wound. Too many
operations are being performed on board ships.
Experienced surgeons were not available for all hospital
ships; their staff was not large, and the rush as at times
very great. 37 During the first two months much major
surgery was due—in respect of time after wounding—to be
done in the "black" ships, where for a time the conditions
were at best difficult, at the worst dreadful. Medical officers,
made responsible for serious cases in overwhelming numbers
which must be held for two days or longer, found themselves
between the devil of dangerous delay and a deep sea of
trouble if severe operations were carried out under circumstances
that made exact procedure and suitable after-treatment
impossible. From the conditions of practice in Australia few
"doctors" were without some operative ability; in the field
ambulances—on which fell the brunt of the work in "black"
ships during the first two months—were many hospital
surgeons, but even for the experienced this was a harsh and
violent introduction to war surgery. Though the severe forms
of wound infection were infrequent, through inadequate
attention and delay ordinary sepsis in severe and deep
wounds was often extensive—even myiasis was not very uncommon.
From the end of June onwards an increasing proportion
of severe cases were carried in the hospital ships.
Gradually also the "black" ships were better staffed; and,
with the introduction in July of the "hospital carrier" and,
of supervision by surgical consultants, surgery in most vessels
approached that performed in the casualty clearing stations
in France, ^ at this stage of the war.
37 The Guildford Castle—with 5 medical officers, 7 nursing sisters, and 38
orderlies—normally took 350 patients, but at times carried up to 520. "On
some trips" (a nurse records) "work was very heavy, we did at least 20 hours
a day. . . I have found patients dead, perhaps for quite a time undiscovered,
not due to neglect but because of shortness of staff. . . What we did was
just like a drop in the ocean to what should have been done."
misdated 29th
28/3/18
Fairweather to 38 Bn
3.15 pm
Our arty very short. Can you have corrected.
Position. In touch with 37th on right, Lancs Fus on left.
No confidence in English troops. Have put several groups
under my own NCO's. Do not consider can advance from wood
without strong fighting. Support my present line be held as
main line.
Enemy actively working on Ridge are in Morlancourt. His M'Gs
snipers active. My casualties 2 wounded, one severely.
Treux Wood
3.15 pm
468 THE GALLIPOLI CAMPAIGN (1915
should not be sutured, and in September the senior consulting
surgeon, M.E.F., found it necessary to repeat that instruction.
The danger of the tourniquet and the superior efficacy, in most
forms of haemorrhage of "direct action" by plugging and
pressure on the wound was a discovery made gradually. The
introduction early in the campaign of the "shell dressing" 34
marked what was almost an epoch in first-aid. No problem
in first-aid was more difficult than that presented by fractures
of the femur, and no surgical treatment was more tragically
futile than that in use. Comparatively few of these terrible
cases reached the base alive on the deadly "long Liston"
splint then in vogue. 35 Thomas splints were not at this time
supplied for field use. The principle embodied therein was,
however, at times applied by regimental medical officers by
extension from each end of the stretcher.
Such of the immediate surgery as was not postponed till
the base hospitals in Egypt were reached was for the most
part carried out at sea in the hospital ships or
Surgery on "black" ships and in hospitals at Lemnos.
board ships The circumstances, therefore, under which it
was done varied greatly. In the hospital ships on the one hand
there was opened up a unique short cut to safety for serious
cases. Of the Guildford Castle, for example, Lieutenant-
Colonel G. A. Syme, A.A.M.C., records "we had the
equivalent of a well-equipped base hospital close to the firing
line." 36 Save in some of the best equipped of these, however,
34 After the Landing, except for local mishaps, there was at no time any
shortage of dressings. The magnitude of the task notably accomplished during
the war by the medical supply department of the War Office can be seen (ex pede
Herculem) from the following items supplied to Gallipoli—namely, "over 4½
million bandages, 3,711 miles of gauze, 374 tons of lint and wool, and 186,000
shell dressings". (Sir Alfred Keogh: evidence given at the Dardanelles Commission.)
35 In The British Medical Journal of January 1915, there had appeared an
illustrated article by Dr. Robert Jones (later Major-General Sir Robert Jones),
of Liverpool, containing the advice given by him to the War Office in 1914 for
splints specially adapted for field use in the war. A pregnant sentence ran as
follows:-
"Upper and lower thighs. In fractiures of the thigh the Thomas knee-splint
is incomparably the simplest and best. I have often fixed a fractured
thigh in this splint and sent the patient home in a cab".
With strange lack of vision, this advice was applied by the War Office only by
way of secondary procedure. Some of these splints were purchased privately by
regimental and other officers in the A.I.F. before and during the Gallipoli
campaign.
36 An account, written by Lieut. -Col. Syme, of surgical work in this fine hospital
ship appears in The Medical Journal of Australia, 1 April, 1916. In the same
journal of 29 January, 1916, useful suggestions for "Transport of sick and
wounded on ordinary troopships" are given by Major A. J. Aspinall, A.A.M.C.
28 March 1918.
Telephone message from 10 Bde to 3 Div. 3.50 p.m.
(from 38 Bn) (officially from 38Bn)
Durham Light Infy occupy line running from N. to S.
through the R in Treux (1/100000 Amiens) thence S
along road turning West along southern edge of wood.
38 Bn are in touch with them in the wood & continue the
line towards the figure 90 (Contour). Boche has taken up
position along spur from figure 60 (Contour) between
Treux & Morlancourt south to immediately south of T
in Post & is actively working on it. Boche active in
Morlancourt also. His m/gs and snipers active.
38 Bn had two men wounded.
524 THE GALLIPOLI CAMPAIGN (Jan, 1915-June, 1916
each district and the pharmaceutical staff officer at headquarters
maintained an effective liaison between the medical
service and the pharmaceutical profession—which by this
time was facing technical problems of considerable complexity
created by the war in connection with the supply of drugs.15
It remains now to follow, from the point of view of the
medical service, the fortunes of the general volunteers of
Outward flow the A.I.F. in the camps of training and
of effectives-- hospital system in their home country.
examination Attention is directed first to the medical
of recruits responsibilities in connection with the troops
for overseas—responsibilities which began
with the medical examination of the recruits. In Australia,
as elsewhere, the first year of the war revealed the fact that
a comparatively large and quite unexpected proportion of
the adult male population was unfit for military service.
Recruiting during the first eighteen months of the war was
marked by a progressive lowering of the physical standards
(in height, weight, and chest measurement) and by increasing
difficulty in complying with the reiterated demands from
the A.I.F. for adherence to a high standard of fitness.
Bombarded from overseas with repeated
Protests from protests at the inclusion of men considered
overseas not unsuitable by medical officers at the front,
fully borne out and impelled on the other hand—as the call
for "effectives" became more clamant and the "first fine
frenzy" for enlisting wore off—by increasing pressure,
political and other, to relax the stringency of the medical
tests, the acting Director-General trimmed a course to suit
both sides, and ended in satisfying neither. It cannot
be said that investigation of the available records of
re-examinations of men returned from overseas as "unfit"
reveals any startling evidence of laxity at this time. It
is true that reports from various sources make it clear
that a considerable number of obviously unfit recruits
slipped through: but the majority of the men concerned in
the iterated complaints from the A.I.F. were the subject of
15The problems, economic and technical, brought about by the dislocation of the
sources of supply of drugs, etc., though of great interest, can only be touched upon
in this work. Certain aspects of the problem will be mentioned in Vol. II of
this history, and Vol. XI of the History of Australia in the War of 1914-1918.
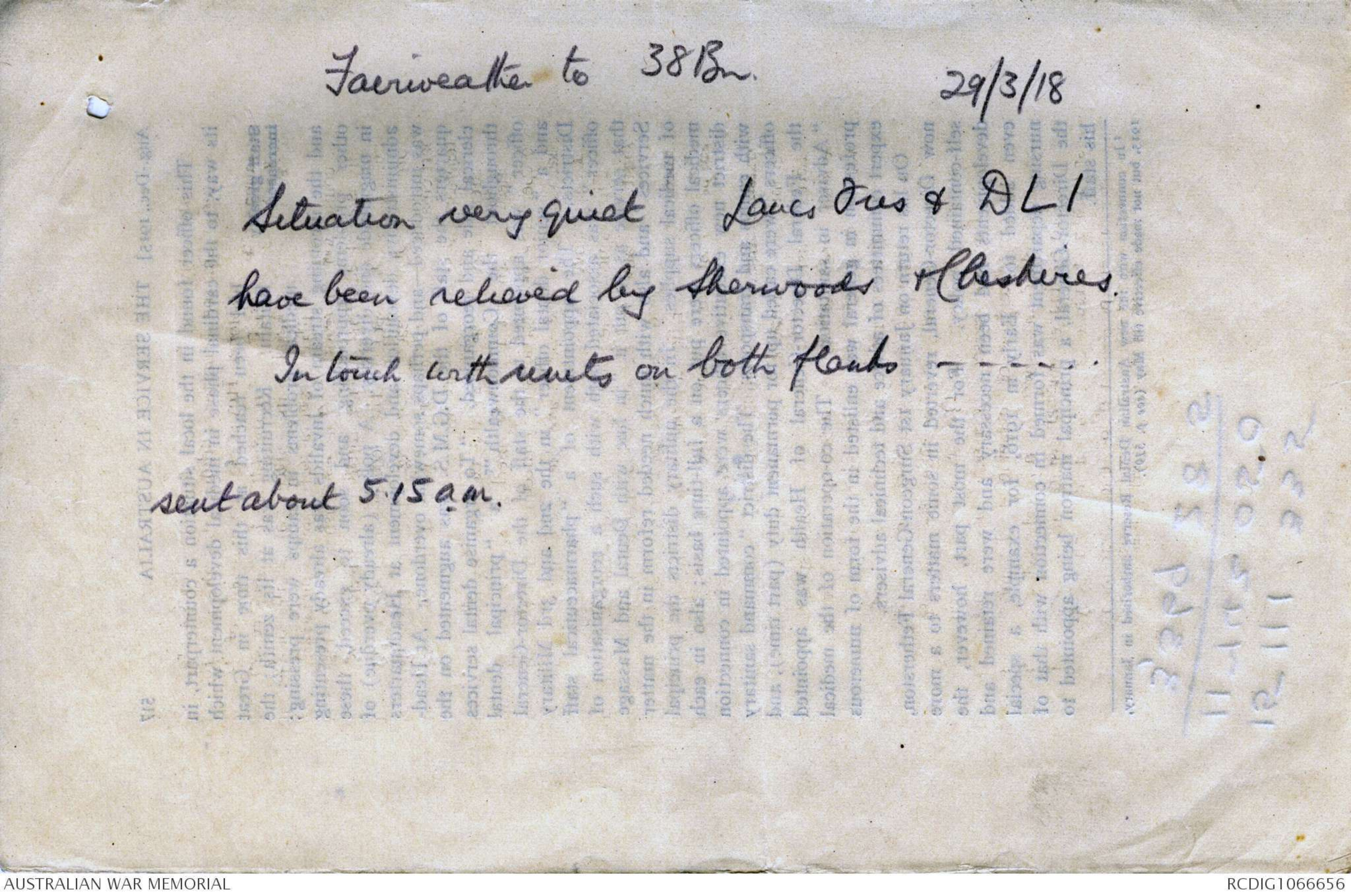
Fairweather to 38 Bn
29/3/18
Situation very quiet Lancs Fus & DLI
have been relieved by Sherwoods & Cheshires
In touch with units on both flanks
sent about 5.15 a.m.
 Sam scott
Sam scottThis transcription item is now locked to you for editing. To release the lock either Save your changes or Cancel.
This lock will be automatically released after 60 minutes of inactivity.